In the rapidly evolving field of longevity science, biomarkers are our compass. They help us navigate the complex terrain of biological aging, acting as indicators of progress or regression in healthspan and lifespan. In 2025, two landmark publications approached the subject from distinct but complementary angles, each attempting to chart a map of aging by identifying the most meaningful biological signposts.
This article offers an in-depth review of those two papers:
- “An Expert Consensus Statement on Biomarkers of Aging for Use in Intervention Studies” (Perri et al., The Journals of Gerontology, Series A)
- “Immunological Biomarkers of Aging” (Wu et al., The Journal of Immunology)
Their methodologies differ. One relies on structured consensus from global experts; the other dives into mechanistic immunology. But together, they represent a critical step toward standardizing how we assess biological age—and how we intervene in it.
The Consensus Approach: Delphi Methodology Meets Aging Science
Perri et al. employed a rigorous and structured process called the Delphi method. This approach is widely used in policy, clinical guidelines, and technology forecasting when empirical consensus is elusive but urgently needed. Their study recruited 460 experts worldwide, drawing from a diverse pool of gerontologists, biologists, clinicians, and public health professionals. The aim was to arrive at a shortlist of aging biomarkers that could be used reliably in intervention studies.
The study proceeded in three rounds:
Round 1 began with an open-ended prompt: “List all biomarkers of aging suitable for use in human intervention studies.” From the 116 expert responses, they gathered over 460 distinct biomarkers.
Round 2 narrowed that list to 20 biomarkers cited by at least ten experts. Each biomarker was evaluated using a 25-item checklist that probed various aspects: reliability, clinical relevance, invasiveness, cost, and whether the biomarker predicted biological age better than chronological age.
Round 3 re-evaluated any biomarkers that didn’t reach consensus in Round 2, allowing participants to adjust their votes in light of group feedback. A biomarker achieved consensus if 70% or more of respondents agreed on its utility.
The results of this process were 14 biomarkers with high consensus. These biomarkers didn’t emerge arbitrarily—they were chosen for their relevance to known hallmarks of aging, their feasibility in clinical settings, and their sensitivity to change following interventions.
Inflammatory Biomarkers:
- Interleukin-6 (IL-6): A well-known cytokine associated with chronic inflammation, IL-6 increases with age and is involved in the development of frailty, sarcopenia, and cardiovascular disease. It is a hallmark of “inflammaging.”
- High-sensitivity C-reactive protein (hsCRP): A stable, widely-used marker of systemic inflammation, hsCRP predicts cardiovascular events and has been linked to overall mortality in older adults.
Physiological Biomarkers:
- Insulin-like Growth Factor 1 (IGF-1): IGF-1 is a mediator of growth hormone activity and plays a crucial role in metabolism, tissue maintenance, and cell proliferation. Low levels are associated with aging phenotypes, but excessively high levels are linked to cancer risk.
- Growth Differentiation Factor 15 (GDF-15): Often elevated in age-related diseases, GDF-15 is a stress response cytokine linked to mitochondrial dysfunction, frailty, and multimorbidity.
Functional Biomarkers:
- Muscle Mass & Muscle Strength: Muscle atrophy is a key feature of aging. Loss of muscle mass (sarcopenia) and reduced strength predict disability, hospitalization, and mortality.
- Handgrip Strength: A simple, yet powerful predictor of frailty and overall health status.
- Timed-Up-and-Go (TUG) Test, Gait Speed, and Standing Balance Test (SBT): These mobility tests assess neuromuscular coordination and risk of falls. They are strongly associated with biological age.
- Frailty Index: A composite measure of vulnerability to stressors, using a deficit-accumulation model.
- Cognitive Health: Typically assessed using tools like the Montreal Cognitive Assessment (MoCA), cognitive decline correlates with biological aging and predicts poor outcomes.
- Blood Pressure: Though a traditional clinical measure, variability in blood pressure and loss of diurnal rhythm are increasingly recognized as signs of vascular aging.
Epigenetic Biomarkers:
- DNA Methylation / Epigenetic Clocks: These clocks, including Horvath’s clock and others, estimate biological age based on methylation patterns at specific CpG sites. They are sensitive to lifestyle interventions and disease states.
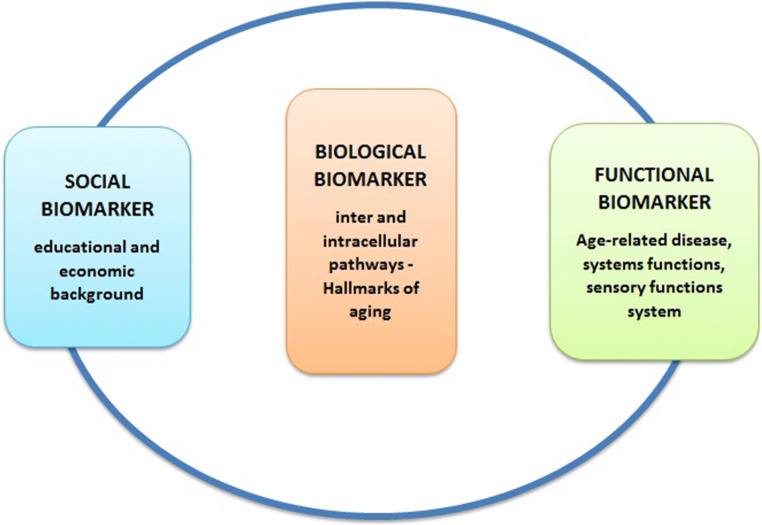
Image from Giuseppe Colloca et al., 2020. PMID: 32827112.
The strengths of this approach lie in its structure, transparency, and broad buy-in. While not all experts agreed on every marker, the final list reflects broad consensus and sets a foundation for standardizing intervention trials.
The Mechanistic Approach: Immune Aging Under the Microscope
Wu et al. approached the question of aging biomarkers through a different lens—immunology. Rather than pursuing consensus, they aggregated and interpreted recent literature on immunosenescence, inflammaging, and age-related immune dysfunction. Their review dives deep into the cellular, molecular, and metabolic shifts that occur in the immune system with age.
Where Perri et al. sought convergence, Wu et al. embraced complexity. They argue that aging cannot be understood without appreciating the immune system’s central role in chronic disease, vaccine response, cancer surveillance, and even neurodegeneration.
Their review identifies several categories of immunological biomarkers:
Cytokines and Soluble Factors:
- IL-6, TNF-alpha, IL-1beta: These pro-inflammatory cytokines are elevated in aging and drive many age-related pathologies, including cardiovascular disease, metabolic syndrome, and Alzheimer’s.
- CXCL9: This chemokine is associated with vascular aging and is a key component of the inflammatory aging clock (iAge).
- IL-10: An anti-inflammatory cytokine that tends to decline with age, contributing to immune imbalance.
Immune Cell Subsets:
- CD28-negative T cells: These senescent-like T cells lose co-stimulatory capacity, accumulate with age, and suppress immune function.
- Age-associated CD8+ T cells (GZMK+, PD-1+): These cells reflect clonal expansion and immune exhaustion, contributing to reduced immune surveillance.
- Age-associated B cells (CD21low, IgD-CD27-): These subsets produce autoantibodies and are linked to autoimmunity in the elderly.
- Regulatory T cells with metabolic shift: These cells skew toward glycolytic metabolism, leading to impaired suppression and heightened infection risk.
Functional and Molecular Readouts:
- Perforin and granzyme secretion: Reduced in NK and cytotoxic T cells, compromising tumor and viral control.
- TCR/BCR diversity: Loss of receptor diversity reflects thymic involution and impaired immune adaptability.
Systems-Level Metrics:
- iAge (inflammatory aging clock): Built using machine learning on over 1,000 blood immune profiles, iAge predicts multimorbidity, frailty, and cardiovascular risk.
- SCENITH (Single-Cell Energetic Metabolism by Profiling Translation Inhibition): A cutting-edge assay to measure immune cell metabolism in real time.
- scRNA-seq-based clocks: These track transcriptomic aging signatures within immune subpopulations, revealing shifts in naïve-to-memory cell ratios and exhaustion markers.
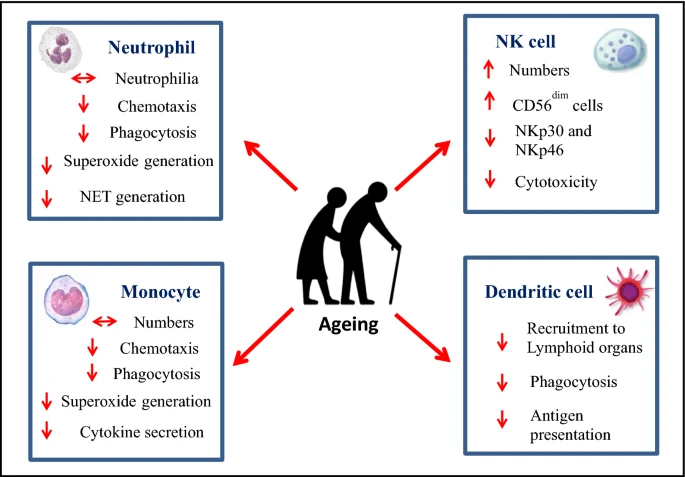
Image Niharika A Duggal, 2018, PMID: 30269199.
This paper’s strength lies in its granularity. While less prescriptive than Perri et al., it underscores that the immune system both reflects and drives aging, and that many changes can be observed directly from peripheral blood.
Comparison and Overlap
While the two papers differ in scope and method, their overlap is revealing. Both highlight IL-6 as a pivotal marker. Perri’s inclusion of hsCRP and IGF-1 also aligns with Wu’s discussion of inflammatory tone and metabolic function.
That said, several markers are notably divergent:
- TNF-alpha, a central player in Wu’s immune narrative, was excluded by Perri’s panel.
- Epigenetic clocks, endorsed by Perri et al., are absent from Wu’s review, likely due to their system-wide rather than immune-specific scope.
- Composite functional measures (e.g., gait speed, cognitive tests) are absent from Wu but prioritized in Perri’s list for their strong clinical predictive value.
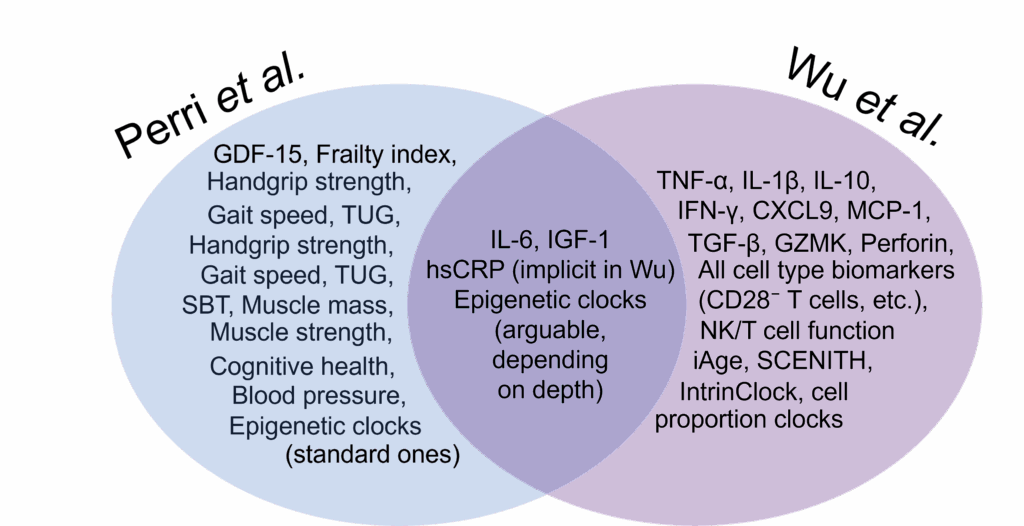
Venn diagram showing the overlapping and non-overlapping biomarkers of aging from the two manuscripts being discussed here.
The overlap matters. IL-6 and hsCRP appear in both discussions and are blood-based, accessible, and prognostic, making them ideal candidates for near-term clinical adoption. Where the two studies diverge, we see the natural tension between what is currently validated versus what is mechanistically insightful.
What They Missed: Biomarkers for the Next Generation
While both papers are rich in insight, several emerging or underutilized biomarkers deserve mention:
- Glycan Age: IgG glycosylation patterns predict immune aging and inflammation. Glycan age correlates with chronological and biological aging and responds to diet and exercise interventions.
- Senescence-Associated Secretory Phenotype (SASP): Beyond IL-6 and TNF-alpha, SASP includes factors like PAI-1, MMPs, and extracellular vesicles that signal tissue-level senescence.
- Mitochondrial DNA (mtDNA) Copy Number/Damage: Mitochondrial dysfunction is a hallmark of aging. Blood-based mtDNA damage reflects oxidative stress and cellular turnover.
- Proteomic Age Clocks: Technologies like SOMAscan allow for high-dimensional plasma proteomics, offering robust age predictions and disease risk stratification.
- Metabolomic Panels: Especially relevant for aging pathways tied to metabolism, these can uncover novel risk factors for insulin resistance, fatty liver, and cardiovascular decline.
These emerging biomarkers reflect the field’s momentum. The goal is not to replace the validated markers, but to build layered composite scores that reflect multiple dimensions of aging.
Final Thoughts
Biomarkers are not just tools; they are strategic assets in the war on aging. Perri et al. give us a roadmap vetted by expert consensus, suitable for trials and regulatory approval. Wu et al. show us the cellular and molecular terrain—messy, dynamic, and deeply revealing.
Where they agree—on IL-6, hsCRP, and IGF-1—we find sturdy ground. Where they diverge, we find inspiration.
The future of aging intervention will be hybrid: consensus-driven enough to be accepted by regulators, and mechanistically insightful enough to push the science forward. These two papers are essential reading for anyone building that future.
Stay tuned, because the next generation of aging clocks might not just measure time—they may help us turn it back.